Hey loyal readers,
In case you're not aware, this has been a crazy month at the Office of HIV Planning. We held two emergency meetings, where very important decisions were made. I'll explain them in detail in my next blog post, but I need a little extra time to do it. This month's "Big Picture" post will go up on Monday, and that's when our email newsletter will go out too.
In the meantime, check out Nicole's very informative post on linkage to care research (you can find it at http://hivphilly.blogspot.com/2013/03/the-science-linkage-to-care.html). There's also a new infographic over at the Kaiser Family Foundation on the impact of Medicaid expansion and non-expansion on low-income people at http://jama.jamanetwork.com/article.aspx?articleid=1672246.
As always, let us know if you have any questions, and see you on Monday!
Briana
Thursday, March 28, 2013
Thursday, March 21, 2013
The Science: Linkage to Care
Linkage to care is a hot topic these days. It sounds so simple, help newly-diagnosed people get into HIV care within 30-90 days (time period depends on who does the measuring). But like with so many other things, it isn’t always that simple. Humans are complex social creatures with needs, fears, beliefs, values, desires, and experiences. These factors play a big part in whether or not a person enters HIV care right away, or at all.
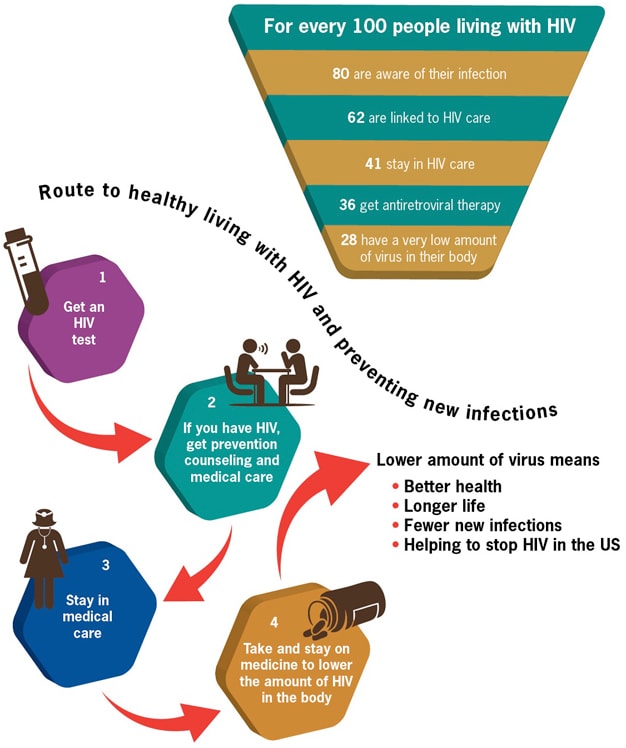
Before we go any further talking about linkage to care, we should make sure everyone understands that linkage to care is just one stop along the continuum of HIV care, as shown on the CDC’s image above and famously described by Gardner, McLees, et. al (2011). You can also check out this short Prezi to get context for the importance of linkage to care.
This was a small qualitative study of patients at a clinic in Mississippi.
Barriers:
Of the 513 MMP participants in 2007-2008, 23% had delayed entry in to care longer than three months after diagnosis. Two independent factors of delayed entry included an earlier year of diagnosis and testing in a nonmedical setting. Of the 28 NIC participants, over half had tested positive in a nonmedical setting. The primary reasons for delayed entry into care for both NIC and MMP were denial of HIV status and not perceiving a need for medical care.
eHIV Review Podcast, Vol 1, Issue 4 (Transcript)
Featured Cases: Linkage and Retention in HIV Medical Care by Dr. Michael Mugavero
Before we go any further talking about linkage to care, we should make sure everyone understands that linkage to care is just one stop along the continuum of HIV care, as shown on the CDC’s image above and famously described by Gardner, McLees, et. al (2011). You can also check out this short Prezi to get context for the importance of linkage to care.
The CDC reports that about 80% of all people with HIV are aware of their HIV status, and only 62% are linked to care. That means that 62% of all the people in the United States who have HIV have had one HIV medical appointment. So that means 38% have not.
One way to improve our practice and service planning is to review the social science to see what researchers have found to be barriers and facilitators (things that help) to linkage. Factors vary and include individual, provider and systemic characteristics. Examples include stigma, denial, substance abuse, place of HIV testing, insurance status, health beliefs about HIV, and other socio-economic, psycho-social and provider-related concerns. Below you will find short summaries of two of the many research articles and resources related to linkage to care, followed by two more resources by Dr. Michael Mugavero (an expert on linkage and retention) to get more information.
Qualitative Assessment of Barriers and Facilitators to HIV Treatment by Bryman Williams, K.R. Amico, and D. Konkle-Parker in the Journal of the Association of Nurses in AIDS Care, 2011
This was a small qualitative study of patients at a clinic in Mississippi.
Barriers:
- Competing demands (family, jobs, childcare)
- Care system aspects (quality of care, access to care, privacy)
- Stigma
- Experience of negative effects (fear of abandonment, hopelessness, denial)
- Various beliefs about the need for or the role of HIV treatment
Factors that helped linkage and retention:
- Support (navigators, family, friends, support groups, clinic staff)
- Investment in one's own care (acceptance, empowerment, knowledge of HIV, monitoring labs, etc.)
- Positive aspects of the health care visit (relationship with provider, being assured of the best treatment)
- Perceived vulnerability of negative consequences of not keeping up with treatment (fear of progression to AIDS, avoiding drug resistance, death)
Social support was the factor most often mentioned by participants, because it was believed to have the biggest impact on the patient's motivation to seek appropriate care. Competing needs and responsibilities are a main reason people miss care appointments. These competing needs are particularly influential for lower income PLWHA who may not have access to resources or support to meet competing needs and attend appointments.
Delayed Entry into HIV medical care after HIV diagnosis: Risk factors and research methods by Samuel Jenness, J. Myers, A. Neaigus, J. Lulek, M. Navejas and S. Raj-Singh, 2012
Study data from New York City's Medical Monitoring Project (MMP) dataset (2007 and 2008), part of the larger CDC (and partners) surveillance project and the Never in Care (NIC) study.
Other articles and resources on linkage and retention in care
Predictors of Late Linkage to Medical Care After an New HIV Diagnosis by Michael J. Mugavero. (A part of the Medscape Education series on HIV)eHIV Review Podcast, Vol 1, Issue 4 (Transcript)
Featured Cases: Linkage and Retention in HIV Medical Care by Dr. Michael Mugavero
Monday, March 11, 2013
Health reform resources
This post is a result of a conversation during the March Finance Committee meeting. We were discussing how difficult planning is in the age of health reform (the Affordable Care Act or ACA), sequesters, and continuing resolutions. If you have no idea what I'm talking about, read my last blog post and then come back to get some other sources for reliable and essential explanations on health reform. Here's a primer on the ACA and Ryan White Program, if you need a refresher.
The links below are the sources I go to most often. Please leave links to your favorite resources in the comments.
If you don't know what an RSS feed is or how to use it, check this out before you go any further. RSS feeds are your friend for access to the latest information with little to no effort. I love Google Reader, here's a short video on how to use it.
The NJ For Health Care Campaign is made up of a broad-based alliance of health care, consumer, senior, student, disability, women's, labor, faith-based, civil rights and social justice organizations working to bring guaranteed, high quality, affordable health care to all New Jersey residents. Resources include a report on the impact of the ACA on NJ's families.
The links below are the sources I go to most often. Please leave links to your favorite resources in the comments.
If you don't know what an RSS feed is or how to use it, check this out before you go any further. RSS feeds are your friend for access to the latest information with little to no effort. I love Google Reader, here's a short video on how to use it.
Health Reform
Kaiser Family Foundation
Kaiser Family Foundation is one of the best sources for all things related to health policy. The outstanding health reform section includes interactive content, videos, charts and graphs, and reports. I highly recommend subscribing to some Kaiser email newsletters for the latest news on health policy. You can also subscribe to RSS feeds of their content.
Other useful content from Kaiser Family Foundation:
Kaiser also provides great fact sheets for different topics or issues, including HIV.
They also wrote an excellent report on Medicaid and HIV.
Other useful content from Kaiser Family Foundation:
Kaiser also provides great fact sheets for different topics or issues, including HIV.
They also wrote an excellent report on Medicaid and HIV.
Commonwealth Fund
Commonwealth Fund is a private foundation focused on improving the quality of our health system. They have a nice interactive health reform timeline and a resource tool for searching for particular topics. You can also subscribe to email newsletters and RSS feeds for regular updates.
This national consumer advocacy organization dedicated to realizing high-quality, affordable health care for all Americans is a well respected voice in health policy circles.
Navigators and Exchange Assisters are going to be needed as the ACA is fully implemented. Find out how you can get ready to implement a navigator/assister program.
Medicaid Defense Center
This section highlights what's happening in Washington and the impact on Medicaid,includes resources for advocacy at a state and national level.
Sign up for the email updates and if you include your state in your contact information you will get state-specific information and resources.
Navigators and Exchange Assisters are going to be needed as the ACA is fully implemented. Find out how you can get ready to implement a navigator/assister program.
Medicaid Defense Center
This section highlights what's happening in Washington and the impact on Medicaid,includes resources for advocacy at a state and national level.
Sign up for the email updates and if you include your state in your contact information you will get state-specific information and resources.
Healthcare.gov
The federal government created this resource for consumers and small businesses to learn about enrollment in the new insurance products and how health reform affects individuals and families.HIV and Health Reform
HRSA: Ryan White and the Affordable Care Act
HRSA just announced (3/5/2013), a new web source for information on the relationship between health reform and Ryan White, including a comprehensive review (PDF) of the key provisions of the ACA for the Ryan White Program.
HIV Health Reform
This site is the go-to source for HIV-specific health reform information. They offer webinars, fact sheets, email alerts, and have a blog. There is also a section written for people living with HIV.
This organization is dedicated to providing education and capacity bulding to improve HIV care and prevention services. Webinars are offered for Ryan White providers, primary care providers and other organizations. They also have an RSS feed and other ways to keep up to date on their work.
Impact on Health Reform in PA and NJ
State Essential Health Benefits Benchmark Plans
Center for Medicaid and Medicare Services (CMS) lists the summaries of state essential health benefits plans, including a short explanation.
Pennsylvania Health Access Network
This coalition of several PA health and consumer advocates offers PA-specific information on health access and equality issues, including a blog.
PHLP is a nationally recognized expert and consultant on access to health care for low-income consumers, the elderly, and persons with disabilities. Learn about how health reform impacts Pennsylvanians.
Thursday, March 7, 2013
The Spotlight: Ryan White Funding Update
If you are
confused about Ryan White Program funding and how the sequester will affect our
local HIV care system, you are not alone. I hope this post provides you with
some information and resources that alleviate some uncertainty and provide
context for the Planning Council's work.
Ryan White Reauthorization
The Ryan White HIV/AIDS
Treatment Extension Act (2009) expires this fall, but this does
not mean that the Ryan White Program will discontinue. Congress can
(and will) appropriate funds to the Program, even if the Act is not
reauthorized. The previous reauthorizations of the Act had sunset provisions,
which meant that if the law was not reauthorized by a set date, Congress
would not be able to appropriate funds and the program would end. The
sunset provision is not a part of the current act.
 |
| Presdent Obama and Ryan White's mother at the signing of the 2009 reauthorization |
Community
advocates and federal partners agree this is not the best time to seek
reauthorization, because of the current fiscal crisis and lack of bipartisan
Congressional support of health reform. They feel it is too risky to call
attention to an HIV-specific health care law; some members of Congress may
believe such a program is no longer needed in the era of health reform. Congressional understanding of the program varies.
Many members of Congress are new to the job this year (12
Senators and 67 representatives) and they need to be educated on the importance of
the Ryan White Program before we can ask them to think about reauthorization.
The CAEAR Coalition and NASTAD provide regular updates on Ryan White Program funding and policies.
Sequester
Because Congress
didn't compromise on federal budget reduction in January, the sequestration
of funds or sequester was triggered. This
means an automatic, across-the-board 5.1% cut to every discretionary line item
in the federal budget, excluding entitlements like Social Security and
Medicaid/Medicare. As outlined in a report issued by the White House, the
sequester cuts funding for HIV testing, HIV treatment, and research efforts. It
also cuts funding to the states (Pennsylvania and New
Jersey fact sheet) and the Philadelphia EMA, in more programs than
just Ryan White. We are anticipating at least a 5.1% cut to the
Ryan White program, but this is not a certainty. We could lose more or
less funding. We will not know until later this year (see the
discussion below on the funding for FY2013 and the continuing
resolution). The sequester will
not go away after this year. It affects the next decade of federal budgets,
unless Congress and President Obama come up with an alternative plan.
The Bipartisan Policy Center has a great guide on the sequester.
Ryan White Funding FY2013 (started March 1, 2013)
Not only are we
dealing with a sequester, but we also have a continuing
resolution. A continuing resolution is a common way for Congress to
avoid a formal appropriations process, and just carryover the budget from one
year to the next. The continuing resolution can be for one year, six months, or
any other period of time. We are currently working under a continuing
resolution that ends on March 27th. If Congress does not pass
another continuing resolution or pass appropriation bills before then, we could
face a federal government shut down like we saw in 1996 and 1997. President
Obama and Congressional leaders don’t want a shutdown, so it is likely we will
have another continuing resolution. Funding might be
"level" to the Ryan White Program for 2013, BUT would still have a 5.1% cut from
the sequester.
Level funding to the Ryan White Program nationally does not mean the Philadelphia Eligible Metropolitan Area (EMA)
will receive a grant award equal to FY2012’s award. Our EMA’s Part A grant award
is based on two awards - a formula
award based on living HIV and AIDS cases and a supplemental award based on the grant application’s score. In planning
for FY 2013 and beyond, we are anticipating AT LEAST a 5.1% ($1.1 million) decrease in Part
A funding to the EMA. This reduction
in funding will carry over into the FY 2014 allocations process that we are just
beginning. This is also why the Planning Council decided to base the EMA’s FY2013
budgets on the 5% decrease scenarios from last
summer’s planning process.
Matthew McClain’s presentation
from the February 2013 Planning Council meeting offers additional information
and resources about domestic HIV policy.
Subscribe to:
Comments
(
Atom
)