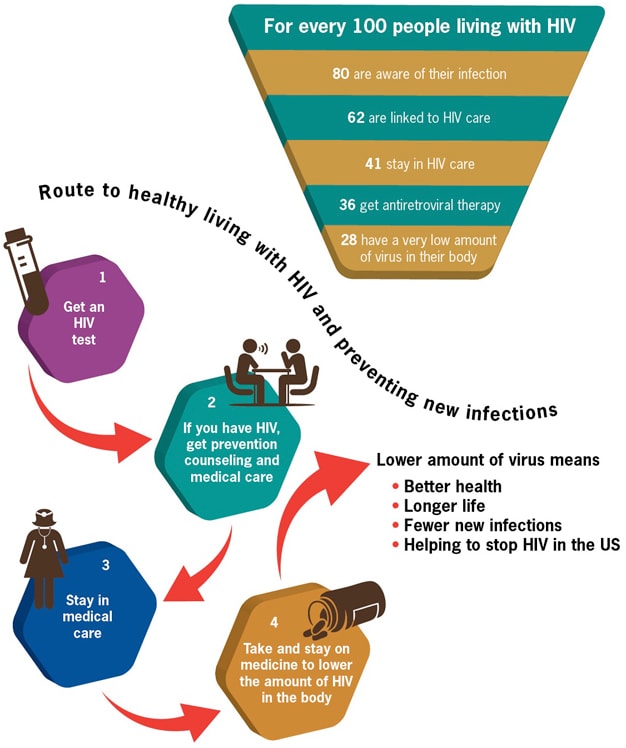
Before we go any further talking about linkage to care, we should make sure everyone understands that linkage to care is just one stop along the continuum of HIV care, as shown on the CDC’s image above and famously described by Gardner, McLees, et. al (2011). You can also check out this short Prezi to get context for the importance of linkage to care.
The CDC reports that about 80% of all people with HIV are aware of their HIV status, and only 62% are linked to care. That means that 62% of all the people in the United States who have HIV have had one HIV medical appointment. So that means 38% have not.
One way to improve our practice and service planning is to review the social science to see what researchers have found to be barriers and facilitators (things that help) to linkage. Factors vary and include individual, provider and systemic characteristics. Examples include stigma, denial, substance abuse, place of HIV testing, insurance status, health beliefs about HIV, and other socio-economic, psycho-social and provider-related concerns. Below you will find short summaries of two of the many research articles and resources related to linkage to care, followed by two more resources by Dr. Michael Mugavero (an expert on linkage and retention) to get more information.
Qualitative Assessment of Barriers and Facilitators to HIV Treatment by Bryman Williams, K.R. Amico, and D. Konkle-Parker in the Journal of the Association of Nurses in AIDS Care, 2011
This was a small qualitative study of patients at a clinic in Mississippi.
Barriers:
- Competing demands (family, jobs, childcare)
- Care system aspects (quality of care, access to care, privacy)
- Stigma
- Experience of negative effects (fear of abandonment, hopelessness, denial)
- Various beliefs about the need for or the role of HIV treatment
Factors that helped linkage and retention:
- Support (navigators, family, friends, support groups, clinic staff)
- Investment in one's own care (acceptance, empowerment, knowledge of HIV, monitoring labs, etc.)
- Positive aspects of the health care visit (relationship with provider, being assured of the best treatment)
- Perceived vulnerability of negative consequences of not keeping up with treatment (fear of progression to AIDS, avoiding drug resistance, death)
Social support was the factor most often mentioned by participants, because it was believed to have the biggest impact on the patient's motivation to seek appropriate care. Competing needs and responsibilities are a main reason people miss care appointments. These competing needs are particularly influential for lower income PLWHA who may not have access to resources or support to meet competing needs and attend appointments.
Delayed Entry into HIV medical care after HIV diagnosis: Risk factors and research methods by Samuel Jenness, J. Myers, A. Neaigus, J. Lulek, M. Navejas and S. Raj-Singh, 2012
Study data from New York City's Medical Monitoring Project (MMP) dataset (2007 and 2008), part of the larger CDC (and partners) surveillance project and the Never in Care (NIC) study.
Other articles and resources on linkage and retention in care
Predictors of Late Linkage to Medical Care After an New HIV Diagnosis by Michael J. Mugavero. (A part of the Medscape Education series on HIV)eHIV Review Podcast, Vol 1, Issue 4 (Transcript)
Featured Cases: Linkage and Retention in HIV Medical Care by Dr. Michael Mugavero
Many people don't believe that it will ever happen to them. They don't educate themselves. They bypass news articles on the subject.
ReplyDeleteWhile it is true that linkage to care is only one step it is also the first step. Without being linked to care you can't be retained in care and you never reach viral suppression. But the point is important to remember as we often become fixated on only one aspect instead of taking into view the entire picture. The cascades show us that, even after all the time and money spent on HIV care we have a long way to go. Let's hope that we use the cascade and other tools to begin to target all of the areas where we can do a better job. This is one of the things we are doing in New York state as we work to improve both linkage to care and retention in care. We note our progress in our own blog which can be found at linkandretain.wordpress.com. We hope some of you will follow along with us there as we post our progress.
ReplyDeleteThanks, Steven! We've shared the link to your blog with our networks, and I've got it in my RSS feed. We have our Points of Integration Workgroup (a joint venture of the Philadelphia EMA Ryan White Planning Council and the Philadelphia HIV Planning Group) working on these issues right now, and the prevention system here currently has an RFP out for ARTAS. Looking forward to keeping up with your efforts!
Delete